
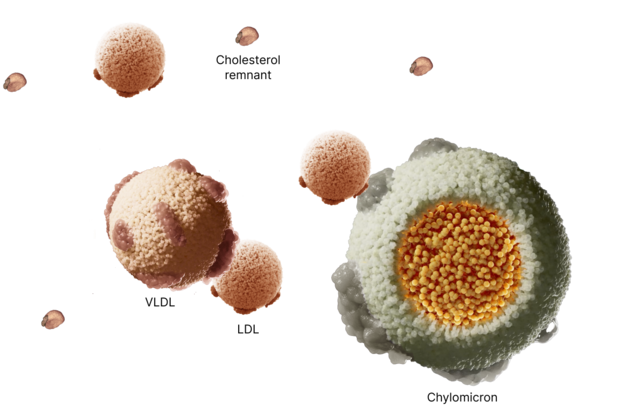
Due to the accumulation of atherogenic lipoproteins seen in levels of ≥500 mg/dL including smaller cholesterol remnant particles, intermediate-density lipoprotein (IDL), and very low-density lipoprotein (VLDL), ASCVD risk increases when triglyceride levels reach 500 mg/dL and above.1,4
The role of lipoproteins
The risks associated with severe hypertriglyceridemia (sHTG) vary depending on the triglyceride level range1-3

≥500 mg/dL
Risks and lipoproteins at this level
Atherosclerotic cardiovascular disease (ASCVD), due to the presence of cholesterol remnant particles, intermediate-density lipoprotein (IDL), and very-low-density lipoprotein (VLDL)—and acute pancreatitis (AP), due to the presence of chylomicrons.1,4
Acute pancreatitis risk
The risk of potentially life-threatening acute pancreatitis (AP) associated with severe hypertriglyceridemia (sHTG) is serious and requires urgent action5
Increased risk for AP is observed with triglyceride levels 500 mg/dL and above and worsens as levels continue to rise1,6,7
*Based on Endocrine Society clinical practice guidelines, elevated triglycerides were defined as serum TG levels ≥150 mg/dL.5
sHTG-induced AP by the numbers
Mortality rate as high as
8%5,8
Prolonged hospitalization of around
17 days5
Healthcare-related costs averaging
$25,000in total mean all-cause costs in the 12 months following AP9
Preventing the first episode of AP is critical10
Once a patient with sHTG has had an episode of AP, their risk of another episode can be

Each subsequent event of AP after the first episode increases the risk of a future attack.10
Atherosclerotic cardiovascular disease risk
Severe hypertriglyceridemia (sHTG) substantially increases a person's risk of ather
osclerotic cardiovascular disease (ASCVD)1,11
Patients with sHTG are

as likely to have ASCVD compared with patients with normal triglyceride levels11
sHTG is independently associated with coronary heart disease (CHD)12
In a real-world study, the rate of CHD events was significantly higher in patients with sHTG compared with those who had normal triglyceride levels at baseline.12*
Rate of CHD events in patients with sHTG at baseline:
16.2%

Rate of CHD events in patients with normal triglyceride levels at baseline:
9.5%
The rate of new CHD events remained statistically significant at follow-up 11.3 years later.
*95% CI, 1.32-2.58; P<0.001.
sHTG requires immediate attention to reduce the risk of ASCVD.11
Other risks
The full mental and physical impact of severe hypertriglyceridemia (sHTG) on patients may be underestimated13
Patients with sHTG report experiencing emotional, cognitive, and physical difficulties13,14
Emotional, cognitive, and physical symptoms were reported in a 6-month prospective observational study of adults with sHTG,13* and in a qualitative interview study of patients with sHTG who had experienced at least 1 episode of AP in the past 2 years.14† These aligned with Patient-Reported Outcomes Measurement Information System (PROMIS) scores below population norm.‡
Emotional
Cognitive
Physical
*
A 6-month prospective observational study of US-based adults with sHTG to evaluate disease burden and treatment patterns based on app-based home-reported outcomes. Monthly in-app surveys were used to collect data on overall health and health-related quality of life, including PROMIS Cognitive Function.13
†
A qualitative interview study of adults with sHTG, very severe HTG, and/or FCS to explore the patient experience of hypertriglyceridemia-related AP. Participants experienced at least 1 episode of AP in the past 2 years requiring an overnight hospitalization. Participants completed a background questionnaire, the EQ-5D-5L (a generic health-related quality of life questionnaire), and select items from a PROMIS profile prior to interview.14
‡
PROMIS is a system of standardized, patient-reported measures for assessing physical, mental, and social health in adults and children, used to measure health symptoms and health-related quality of life domains.15
In US adults with sHTG, up to
The prevalence of hepatic steatosis is 3-fold higher in sHTG than in the general population16
Elevated triglycerides were identified as a potentially important factor that may be causally involved in the onset of MASH in a large-scale metabolomics study17
Addressing sHTG is an important priority for the overall health of your patients.18
References
References
- Virani SS, Morris PB, Agarwala A, et al. 2021 ACC expert consensus decision pathway on the management of ASCVD risk reduction in patients with persistent hypertriglyceridemia: a report of the American College of Cardiology solution set oversight committee. J Am Coll Cardiol. 2021;78(9):960-993.
- Yuan G, Al-Shali KZ, Hegele RA. Hypertriglyceridemia: its etiology, effects and treatment. CMAJ. 2007;176(8):1113-1120.
- Rashid N, Sharma PP, Scott RD, Lin KJ, Toth PP. Severe hypertriglyceridemia and factors associated with acute pancreatitis in an integrated health care system. J Clin Lipidol. 2016;10(4):880-890.
- Ginsberg HN, Packard CJ, Chapman MJ, et al. Triglyceride-rich lipoproteins and their remnants: metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies—a consensus statement from the European Atherosclerosis Society. Eur Heart J. 2021;42(47):4791-4806.
- Nawaz H, Koutroumpakis E, Easler J, et al. Elevated serum triglycerides are independently associated with persistent organ failure in acute pancreatitis. Am J Gastroenterol. 2015;110(10):1497-1503.
- Laufs U, Parhofer KG, Ginsberg HN, Hegele RA. Clinical review on triglycerides. Eur Heart J. 2020;41(1):99-109c.
- Shemesh E, Zafrir B. Hypertriglyceridemia-related pancreatitis in patients with type 2 diabetes: links and risks. Diabetes Metab Syndr Obes. 2019;12:2041-2052.
- D'Erasmo L, Di Costanzo A, Cassandra F, et al. Spectrum of mutations and long-term clinical outcomes in genetic chylomicronemia syndromes. Arterioscler Thromb Vasc Biol. 2019;39(12):2531-2541.
- Rashid N, Sharma PP, Scott RD, Lin KJ, Toth PP. All-cause and acute pancreatitis health care costs in patients with severe hypertriglyceridemia. Pancreas. 2017;46(1):57-63.
- Sanchez RJ, Ge W, Wei W, Ponda MP, Rosenson RS. The association of triglyceride levels with the incidence of initial and recurrent acute pancreatitis. Lipids Health Dis. 2021;20(1):72.
- Arca M, Veronesi C, D'Erasmo L, et al. Association of hypertriglyceridemia with all-cause mortality and atherosclerotic cardiovascular events in a low-risk Italian population: the TG-REAL retrospective cohort analysis. J Am Heart Assoc. 2020;9(19):e015801.
- Saadatagah S, Pasha AK, Alhalabi L, et al. Coronary heart disease risk associated with primary isolated hypertriglyceridemia; a population-based study. J Am Heart Assoc. 2021;10(11):e019343.
- Kessler AS, Zhang C, McStocker S, et al. Study-start characteristics of individuals with severe hypertriglyceridemia (sHTG) in an app-based home-reported outcomes study evaluating disease burden and treatment patterns. Abstract accepted for presentation at: PancreasFest; July 24-25, 2025; Pittsburgh, PA.
- Kessler AS, Aggio D, Howard EM, et al. A qualitative study to explore the patient experience of hypertriglyceridemia-related acute pancreatitis. J Clin Lipidol. Published online April 10, 2025.
- What is PROMIS? PROMIS Health Organization. 2025. Accessed May 14, 2025. https://www.promishealth.org/57461-2/
- Gurevitz C, Chen L, Muntner P, Rosenson RS. Hypertriglyceridemia and multiorgan disease among U.S. adults. JACC Adv. 2024;3(5):100932.
- Gagnon E, Manikpurage HD, Mitchell PL, et al. Large-scale metabolomic profiling and incident non-alcoholic fatty liver disease. iScience. 2023;26(7):107127.
- Kirkpatrick CF, Sikand G, Petersen KS, et al. Nutrition interventions for adults with dyslipidemia: a clinical perspective from the National Lipid Association. J Clin Lipidol. 2023;17(4):428-451.